Thyroid
Thyroid Cancer
Malignant thyroid tumours can be of three types. The most common is differentiated thyroid cancer (90% of the cases) which includes papillary thyroid carcinoma and follicular thyroid carcinoma. These cancers can potentially spread to lymph nodes in the neck and, less commonly, to distant organs like the lungs, but typically have good prognoses if detected and treated early. Medullary Thyroid Carcinoma is less common and can occur sporadically or as part of a genetic syndrome. It originates from the parafollicular cells (C cells) of the thyroid gland. An uncommon but aggressive form of thyroid cancer is Anaplastic Thyroid Carcinoma that often has a poor prognosis due to its rapid growth and resistance to treatment. This form of thyroid cancer is typically found in older patients. Medullary Thyroid Cancer could also be associated with multiple endocrine neoplasia (MEN).
Although thyroid cancer can affect individuals of any age it is more prevalent in women and becomes more common as we get older. It is also more frequent in people who have a history of exposure of the thyroid gland to radiation or a family history of thyroid cancer. But in most patients, the cause cannot be ascertained.
Symptoms may include a visible thyroid lump, swollen neck lymph nodes, hoarseness, and difficulties in swallowing or breathing. Prognosis is typically favourable with prompt diagnosis and appropriate treatment, ensuring good long-term survival outcomes for most patients.


Diagnosis & Treatment
Diagnosis of thyroid tumours usually involves imaging studies such as ultrasound, and biopsy (fine needle aspiration or FNA) to determine whether the tumour is benign or malignant. Regular monitoring and follow-ups are crucial for individuals diagnosed with thyroid tumours to ensure timely detection of any recurrence or progression, and to adjust treatment as needed to optimise outcomes.
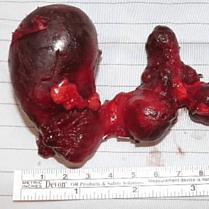
Treatment options depend on the type, size, and location of the tumour. Surgery is the primary treatment for thyroid cancer, with the extent determined by the cancer's stage and type. It may involve removing part or all of the thyroid gland, possibly including lymph nodes in the neck if the cancer has spread.
Radioactive iodine therapy is often used post-surgery for differentiated thyroid cancers to eliminate any remaining cancer cells. This treatment is generally well-tolerated, although precautions are necessary due to temporary radioactivity. Other treatments may include hormone therapy, and in some cases, external beam radiation therapy or chemotherapy.